No products added!
The field of medical aesthetics has undergone a seismic shift, moving from major surgical interventions to minimally invasive procedures that promise immediate rejuvenation. Dermal fillers are at the vanguard of this evolution. Whether using hyaluronic acid, calcium hydroxylapatite, or polycaprolactone, these substances allow practitioners to sculpt, volumize, and revitalize facial structures with remarkable precision.
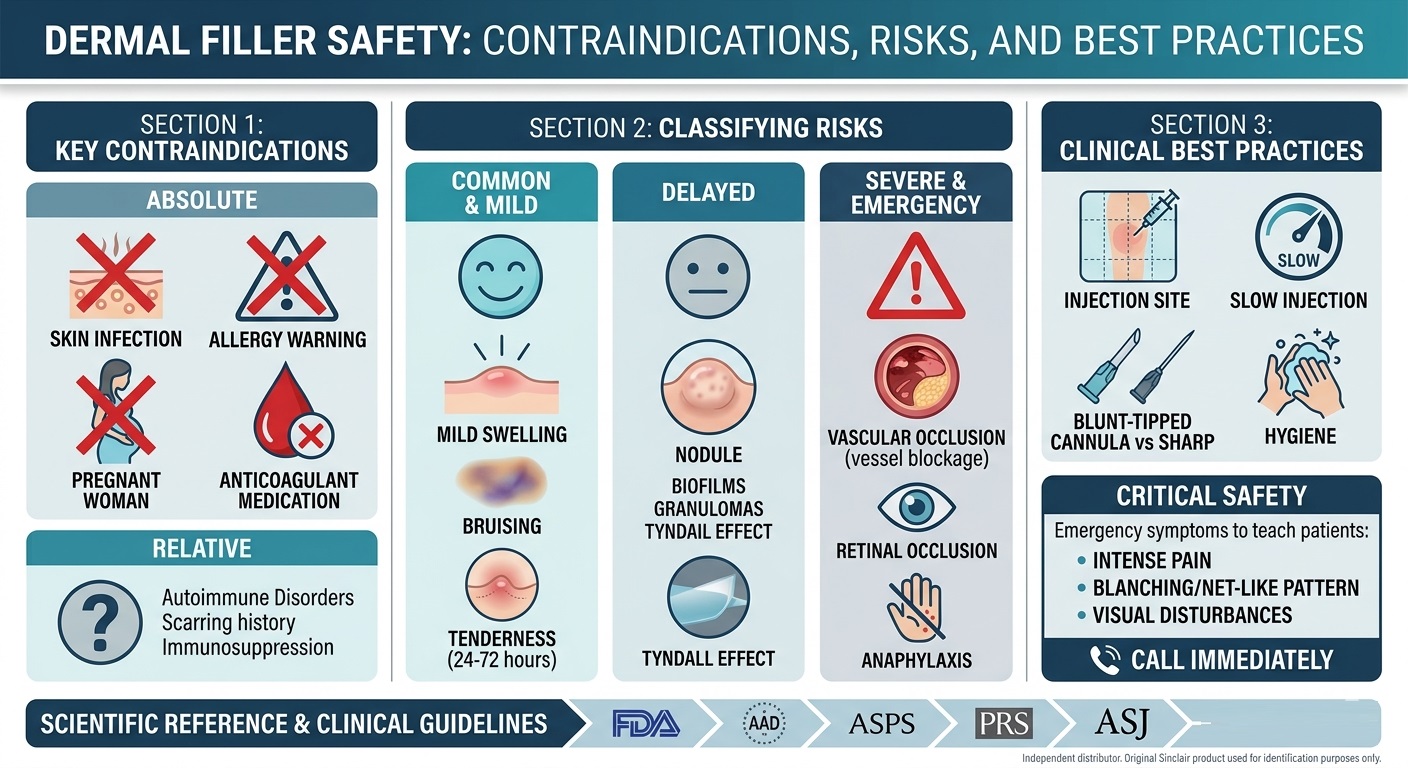
However, the ease of administration often masks the clinical complexity of these procedures. As the market expands, so does the responsibility of the practitioner. Patient safety is not merely about achieving an aesthetic ideal; it is about the rigorous navigation of anatomy, immunology, and material science. This guide synthesizes data from the U.S. Food and Drug Administration (FDA), the American Academy of Dermatology (AAD), and leading plastic surgery journals to outline the landscape of safety, risk management, and clinical best practices.
1. The Regulatory and Clinical Safety Framework
The FDA classifies dermal fillers as medical devices. Their safety and efficacy are predicated on proper use by qualified healthcare professionals. A fundamental rule in aesthetic medicine is that no filler is entirely risk-free.
Understanding the “biomaterial profile” of the product is the first step in safety. Fillers are not interchangeable. Hyaluronic acid (HA) fillers are generally considered “tunable” and reversible via hyaluronidase, whereas semi-permanent biostimulators (such as those containing polycaprolactone) rely on the body’s endogenous tissue response to create volume.
2. Comprehensive Contraindications: Patient Selection
Patient selection is the single most effective tool for preventing complications. Practitioners must distinguish between absolute contraindications and relative contraindications.
Absolute Contraindications
These conditions necessitate the deferral or cancellation of the treatment:
-
Active Infection: Any localized infection (bacterial, viral, or fungal) at or near the injection site (e.g., active herpes labialis) is a strict contraindication.
-
Known Hypersensitivity: A documented history of severe allergy or anaphylaxis to any component of the filler—including the carrier gel (e.g., CMC), the active ingredient (e.g., PCL microspheres), or the anesthetic (e.g., lidocaine).
-
Pregnancy and Lactation: Due to the lack of safety data regarding the effect of filler components on fetal development or breast milk, these treatments should be avoided.
-
Uncontrolled Coagulopathy: Patients with severe bleeding disorders or those on unmanageable anticoagulant therapy present a high risk for hematoma formation and subsequent tissue complications.
Relative Contraindications
These require a detailed discussion with the patient and potentially a consultation with the patient’s primary physician:
-
Autoimmune Disorders: Patients with conditions such as lupus erythematosus or rheumatoid arthritis may exhibit an unpredictable immune response to implanted materials, increasing the risk of granuloma formation.
-
Hypertrophic Scarring/Keloids: A history of pathological scarring suggests an abnormal wound-healing mechanism, requiring a cautious approach.
-
Immunosuppression: Patients who are immunocompromised have a diminished ability to maintain the sterility of the implant site.
3. Classifying Complications: From Common to Critical
Immediate and Mild Reactions
These are the expected sequelae of the procedure:
-
Edema and Erythema: A natural inflammatory response.
-
Ecchymosis: Bruising occurring when a vessel is punctured.
-
Tenderness: Usually subsides within 48 to 72 hours.
Delayed Reactions
These present days, weeks, or even months after the procedure:
-
Biofilm Formation: A low-grade bacterial colonization that can lead to chronic, recurrent inflammation.
-
Granulomas: A foreign-body response where the immune system attempts to “wall off” the product.
-
Tyndall Effect: A bluish discoloration caused by the refraction of light when a filler (typically HA) is placed too superficially.
Severe and Emergency Events
-
Vascular Occlusion (VO): Occurs when filler is injected into a blood vessel or compresses it, starving the tissue of blood (ischemia).
-
Blindness (Retinal Artery Occlusion): A rare but catastrophic event occurring when filler travels retrograde through the ophthalmic artery.
-
Systemic Anaphylaxis: A life-threatening systemic allergic reaction.
4. Clinical Safety Protocols
The literature provided by ASPS (American Society of Plastic Surgeons) highlights that “prevention is better than cure.” The following technical protocols are essential:
-
Anatomical Mapping: A deep understanding of vascular anatomy is mandatory, specifically regarding “danger zones” (glabellar region, nasal bridge, and temple).
-
Aspiration Techniques: Before injecting, the practitioner should aspirate for a few seconds to ensure no blood enters the hub.
-
Low-Pressure Injection: Slow, controlled, low-pressure injection is the standard of care.
-
Hygiene and Sterility: The skin must be cleaned with antiseptic according to a strict, no-touch technique.
5. Recognizing Emergency Symptoms
Patients must be instructed to call the practitioner immediately if they experience:
-
Pain disproportionate to the procedure: Intense, searing pain during injection.
-
Blanching: An area of the skin turns white or pale immediately after injection.
-
Livedo Reticularis: A “marbled” pattern on the skin.
-
Visual Disturbance: Changes in vision or eye pain.
6. Frequently Asked Questions (FAQ)
How can I distinguish between a bruise and a vascular occlusion?
A bruise typically presents as a flat blue/purple discoloration without severe pain. A vascular occlusion presents as “blanching” (white/ashen color) followed by a mottled, purple-red pattern (livedo reticularis), accompanied by intense, increasing pain. If color change persists, treat it as a medical emergency.
What is the role of hyaluronidase in managing complications?
For hyaluronic acid (HA) fillers, hyaluronidase is the antidote. It breaks down the HA and can effectively reverse the blockage in a vascular occlusion. However, hyaluronidase does not work on non-HA fillers (like PCL, PLLA, or Calcium Hydroxylapatite).
Can I perform a touch-up treatment if a patient still has minor swelling?
It is strongly discouraged. Performing additional injections on already inflamed tissue makes it difficult to assess the current volume accurately and increases the risk of infection. Wait at least 2 to 4 weeks.
Why is the glabellar area (between the eyebrows) considered so dangerous?
The glabella has high-density vascular structures (supratrochlear and supraorbital arteries) that have direct connections to the ophthalmic artery. Injecting into these vessels can lead to rapid retrograde flow of the product into the eye’s blood supply, posing a risk of permanent vision loss.
Scientific References & Clinical Guidelines
To ensure the highest standard of clinical practice, refer to these authoritative, peer-reviewed sources:
-
Global Aesthetics Consensus: Avoidance and Management of Complications from Hyaluronic Acid Fillers
-
Source: Plastic and Reconstructive Surgery (PRS). This is the definitive international consensus on managing vascular and inflammatory complications.
-
-
U.S. FDA: Dermal Fillers (Soft Tissue Fillers)
-
Source: U.S. Food and Drug Administration. Official regulatory guidance on device safety, common risks, and patient information.
-
-
Aesthetic Surgery Journal (ASJ)
-
Source: American Society for Aesthetic Plastic Surgery (ASAPS). The official journal providing high-quality clinical studies on new material safety and injection techniques.
-
-
-
Source: American Society for Dermatologic Surgery (ASDS). Essential for understanding dermatological interactions and long-term tissue responses.
-
-
American Society of Plastic Surgeons (ASPS) – Patient Safety
-
Source: ASPS. Clinical resources for surgeons, including safety checklists and best-practice protocols.
-
LEGAL NOTICE: Independent distributor. Original Sinclair product used for identification purposes only.